Report of Oversea Clerkship Program in Osaka Metropolitan University
Clinical Training Report in Osaka Metropolitan University
Lin Yu-Yang
- Country / Regions
- Taiwan
- School
- National Taiwan University(国立台湾大学)
- Elective period
- 21 October to 15 November 2024
Pediatrics
Before the clerkship program started, we had to login to a website called "Moodle" to do the self-evaluation and watch the OSCE video, which was going to be our final exam.
We had case discussion conference in the afternoon of every Monday. The resident doctors had to report the medical history and treatment of all patients in the Pediatric ward to the professor, and sometimes they had to give the presentation of a specific topic such as meconium ileus. After the presentation, each student had been assigned a patient as their primary care case, and I would share the same case with Hayate. Hayate was one of the group members who introduced everything about the school and the hospital to me, and he was also a translator because he could translate what the teacher had taught during the class into English sometimes.
Most of the classes of Pediatrics were in Japanese. I could barely understand the concepts since I could only recognize the meaning of kanji. Nevertheless, I realized that all the classes didn't consist of abundant medical knowledge for students to memorize. The teachers tended to give the introduction of different medical fields to inspire the students' interest. In comparison to the classes I took at the medical school in Taiwan, what I had been taught at Osaka Metropolitan University encourages me to spend more time to study the fields that I was truly interested in rather than memorize all the details of every department.
Hayate and I visited our patient accompanied by the doctors after we got some instructions from them. The chief complaint of our patient was unilateral leg swelling and pain for days, and he was diagnosed with deep vein thrombosis. We had to gather the information of present illness, past medical history, patient's interpretation about his illness, and then we had to perform physical examination to give the tentative diagnosis. I was curious why the patient was admitted to the Pediatric department although he was more than 20 years old, but I didn't ask the professor. Hayate and I presumed the reason was that the patient had congenital disease, which was methylmalonic acidemia. At last, we came up with some diseases that shared similar symptoms with deep vein thrombosis, which were cellulitis, necrotizing fasciitis and thrombophlebitis.
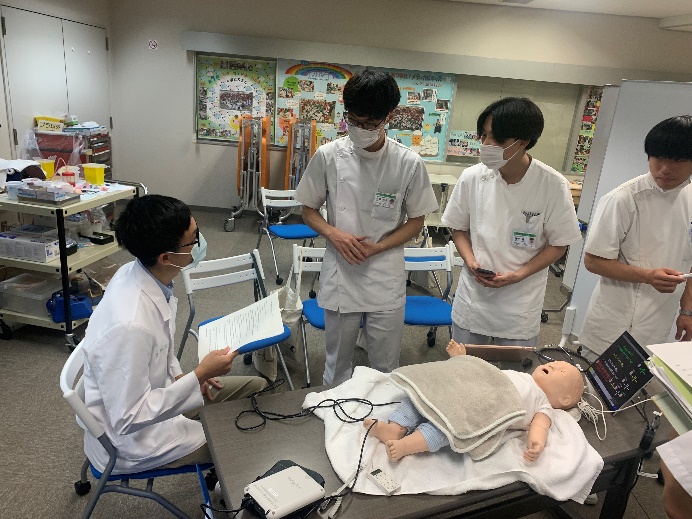
We had the class of blood draw practice class on Friday morning of the first week. The resident doctor demonstrated the steps of blood draw by using the model at Skill Simulation Center. It's my first time practicing this skill, and I failed because we could only try one time. Fortunately, I adjusted the angle and depth of the needle I inserted and succeeded when I had the test with other classmates on Friday afternoon of the second week. That was a special experience for me.

We had a class about OSCE practice on Tuesday afternoon of the second week. The teacher asked each of us to play a role during the practice, which consisted of doctor, nurse, patient's mother, note taker, and timekeeper. We practiced history taking, physical examination and vital signs measurement for 12 minutes. After gathering some useful information about the patient, we had to use these clues for differential diagnosis. At that class, I realized the difference between Taiwan and Japan when it comes to history taking of infants. Medical record in Taiwan focused on birth history, feeding, vaccination, growth and development, allergies, systemic disease, current medication, family history. However, history taking in Japan also put emphasis on triage-related questioning, dehydration risk such as the amount of milk intake, urination, defecation and vomiting, since we couldn't ask the patient directly to get the information that we need.

On the last day, my group members had the OSCE, and I would be the simulation patient. They were divided into two groups, and I had to prepare to cases, which were all conducted in English. Professor 濱崎 wanted to trained the students to acquire the ability to cope with foreign patient. I realized that many Japanese students didn't have the courage to talk to foreigners in English although they may be proficient in English. In addition to answering their questions, I did my best to understand and encouraged them to express what they wanted me to know by body language or even some simple Japanese words. It was a nice and important experience for me to communicate with foreigners, and I hoped it was also meaningful to them.

Neurosurgery
The clerkship program of Neurosurgery was quite different from Pediatrics because we didn't have to submit our homework on the website "Moodle", but we had to join the morning conference at 8 am every day. I believed that the morning conference was important for resident doctors and professors because they could exchange thoughts about the patient's condition before the surgery started.
The morning conference was conducted in English mostly because there were often some neurosurgeons from different countries. I could understand most of the content of the conference, but my group members complained a lot to me. It's because they didn't learn these medical terms in English in the previous classes or textbooks. They had a hard time keeping up with the conversation during the conference.
Each of us was assigned a patient on the first day, and we had to watch his/her operation. I shared the same case with Natsume, and the main diagnosis of our patient was FSHoma. (It was misspelled as "TSHoma" at first.)
Some classed were also in Japanese as I experienced in Pediatrics, but there were two class in English during the two weeks of the clerkship program. They were all Professor 坂本's class, which were how to approach patients related to Neurosurgery, and the mechanism, evaluation and management of brain herniation. I had learned a lot about the typical manifestations of cases of ischemic stroke, hemorrhagic stroke, and tumor-like lesion at the first class. Furthermore, I learned many ways to evaluate the patient's condition who had brain disease at the second class. Professor 坂本 was so kind and enthusiastic that he always explained everything in English for me. We had a lot of interactions, and he indeed inspired my interest in Neurosurgery. I was very thankful for his teaching. At the second class, Professor 坂本 also demonstrated how to measure the head circumference of an infant and the status of anterior fontanelle in all kinds of situations such as sitting, lying supine and crying. It was my first time holding an infant and gently touching the anterior fontanelle. I became more interested in being a pediatric neurosurgeons in the future as Professor 坂本 did after the class.
Since FSHoma meant a tumor in the pituitary gland, the patient would undergo transsphenoidal endoscopic surgery. Natsume and I watched the surgery from 9 am to nearly 4 pm. The professor and the resident doctor performed partial remove of bilateral middle nasal concha, and then removed the wall of sphenoid sinus to create more surgical space. Subsequently, the surgeons drilled out sella turcica and started to remove the tumor. Some tumor lesions were also in the sphenoid sinus. After the surgery, they did duraplasty, mucosal flap, sinus sponge and tissue glue to close the wound. The resident doctor told me one of the most common complications was cerebrospinal fluid leak, so the procedure of wound closure was especially important.
Besides that case, I've watch another operation with 谷澤 on Monday morning of second week. The patient was diagnosed with vestibular schwannoma, so he had to undergo sub-occipital craniotomy to have complete resection of the tumor. The surgeons put lots of effort into remaining right facial nerve intact by using the handheld peripheral nerve stimulator to detect its location. I asked the resident doctor how to differentiate tumor tissue from normal brain tissue, and he answered me that it all depended on the surgeon's experience. I admired them for their expertise and hope I can become such a professional one day.
We practice microscopic suturing on Tuesday afternoon of the second week. My group member experienced this skill for the first time, but I had practiced this about two months ago. I realized that there was still some difference between instrument tie in Taiwan and that in Japan. We tended to wrap the forceps with the suture to make a tie. However, the senior student here taught us to make a circle of the suture and then let the forceps pass through the hole. Both skills were time efficient.
We visited Tsukazaki Hospital on Wednesday of the second week, which was in Hyogo prefecture. The Hospital Director introduced the hospital to us. We saw lots of innovative medical equipment and devices in the operation rooms and examination rooms. In addition, the staff in the hospital could enjoy benefits such as free coffee machines, cheap restaurants and even a child daycare center. They invited us to be a member of them in the future.
The clerkship program of Neurosurgery provided me numerous chances to experience which kind of patients with brain and spine disease they had to take care of, and the environment and life of surgeons. These precious experiences undoubtedly will help me nourish the hope of becoming a great surgeon.